


Resources > Expert Information
National Glaucoma Research
This article discusses primary angle-closure glaucoma, the second most common form of this eye disease. The author discusses important information to know about symptoms, diagnosis, treatment options, known risk factors, and more.
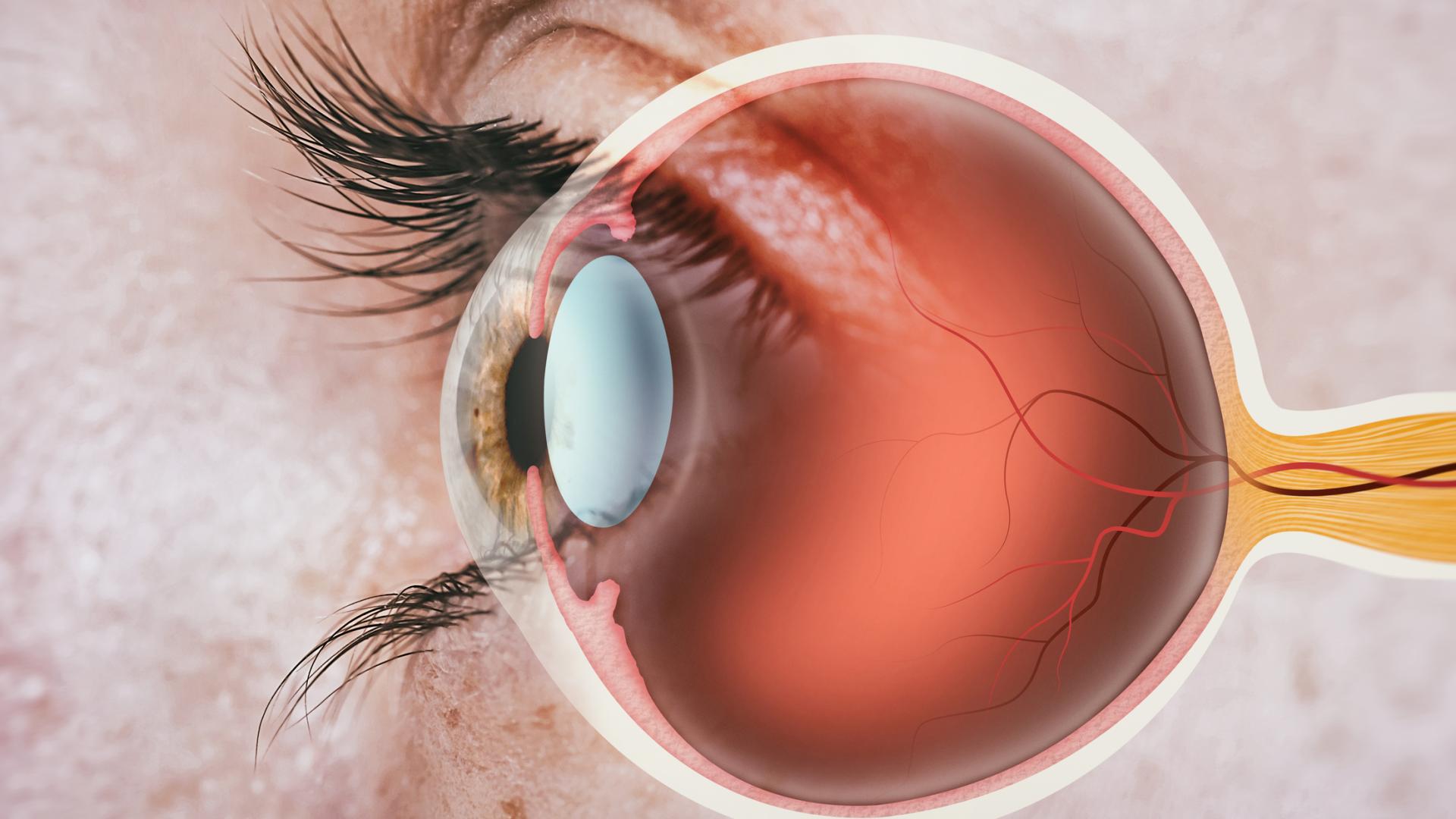
Primary angle-closure glaucoma is associated with closure of the anterior chamber angle of the eye, in contrast to the most common form of glaucoma known as primary open-angle glaucoma. This angle is an important structure in the eye, and is present 360 degrees around the circumference of the eye. The angle can be thought of as the angle between the iris and the cornea, although that is an oversimplification.
Nevertheless, in the angle, one finds the drainage system of the eye, called the trabecular meshwork, which, if your angle is open, is visible to your eye doctor by using a special mirrored lens.
The video below provides a very good representation of the eye’s “angle.”
In primary angle closure, the trabecular meshwork is not as visible because of a “narrowing” of the angle. There are multiple reasons for this “narrowing.”
First, we will define a few more terms. Angle closure may or may not be associated with increased eye pressure or damage to the optic nerve, and can occur in either an acute or chronic form. Indeed, if one has evidence of angle narrowing but no evidence of increased eye pressure or optic nerve damage, your ophthalmologist may diagnose you as a “primary angle-closure suspect.”
If you have angle narrowing and elevated eye pressure, but no optic nerve damage, you may be diagnosed with “primary angle-closure.”
Finally, if you have angle narrowing, elevated eye pressure, and optic nerve damage, you have “primary angle-closure glaucoma.”
Regardless of the exact diagnosis, the risk factors for primary angle-closure glaucoma include:
Other risk factors related to the eye’s anatomy include:
Sometimes angle closure can result in no symptoms, and other times the symptoms are very obvious (as in an acute-angle closure crisis). There can also be intermittent or occasional symptoms, such as blurred vision, halos around lights, eye pain, headache, eye redness, or symptoms occurring after dilation of the eyes. In addition, many medications with glaucoma warnings apply to patients with primary angle-closure. Briefly, these include over the counter decongestants, motion-sickness medications, and anticholinergic agents, just to name a few. Always ask your ophthalmologist about any glaucoma side-effect warnings if you are unsure.
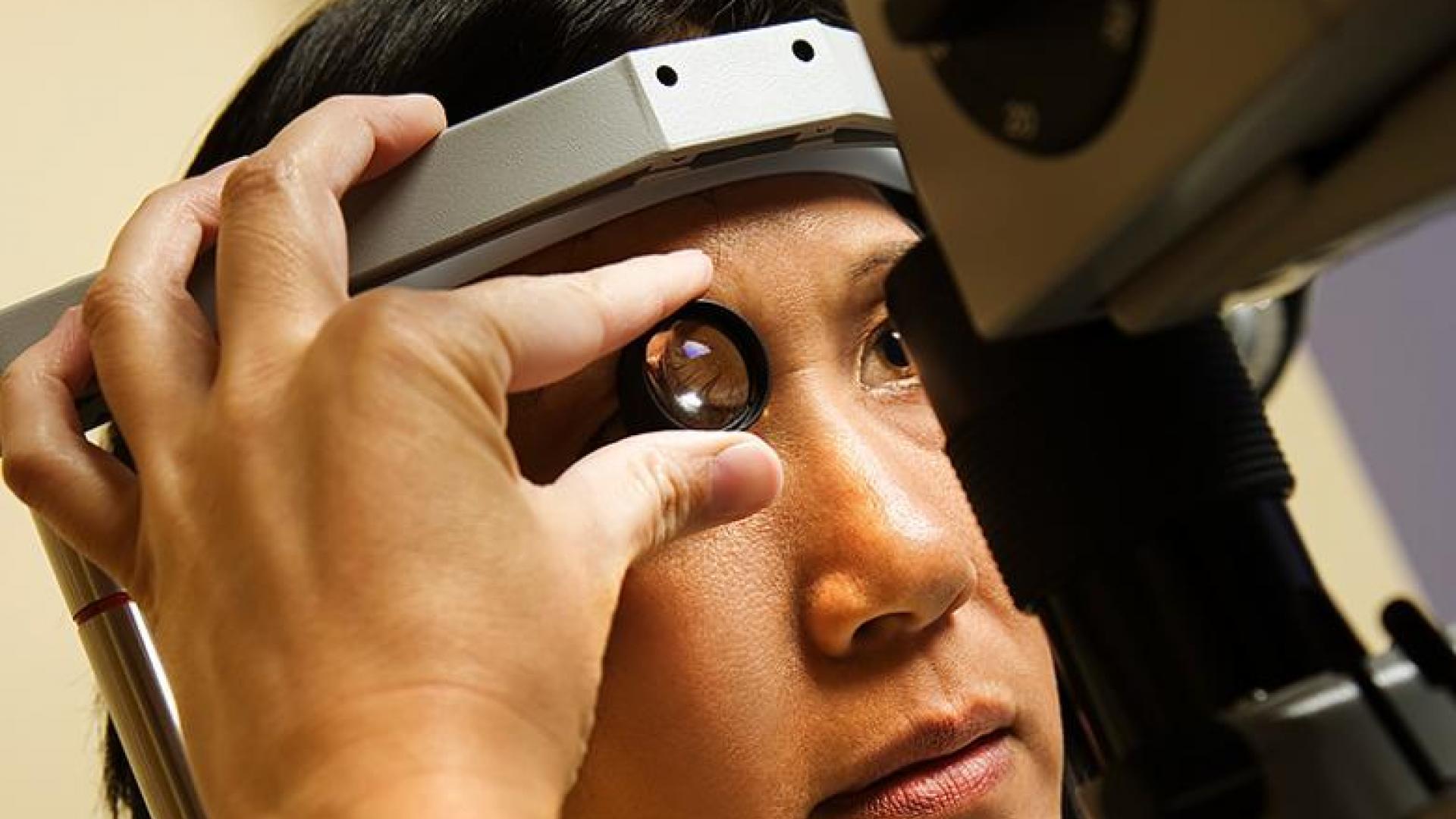
During your eye examination, your eye doctor will assess all parts of the eyes as they would during a comprehensive eye examination, although sometimes a dilated exam will not be performed if your ophthalmologist is very concerned about the narrowness of your angles. In addition, your doctor will perform gonioscopy, which uses a special mirror in order to visualize the angle. Sometimes, imaging of the front part of the eye, called anterior segment optical coherence tomography are, or ultrasound biomicroscopy (a special type of ultrasound eye exam) will be performed to more specifically determine the anatomy of the angle.
After your eye examination, your ophthalmologist will discuss any recommendations for laser peripheral iridotomy, medications, or surgery, which will briefly be discussed below.
In an acute-angle closure crisis, the eye pressure can increase rapidly and to high levels. The patient may experience symptoms such as blurred vision, halos around lights, eye pain, headache, nausea, and possibly vomiting. Untreated, an acute angle-closure crisis can cause permanent vision loss or blindness. In addition, the other eye is at high risk for having a similar crisis. This is why laser peripheral iridotomy is recommended both as a treatment during an acute crisis and in patients who are asymptomatic, but have primary angle closure and are at risk for an acute angle-closure attack.
A laser iridotomy (see video) creates a hole in the iris, which acts as an alternative channel through which eye fluid can flow when the usual pathway becomes blocked.
The risks of the laser iridotomy are relatively low, whereas the harm that an attack can do is relatively high and potentially permanent. In terms of treatment, the initial steps are to break the attack, which will be accomplished using a combination of eye pressure lowering medications and laser iridotomy.
Sometimes removing the lens (or cataract) is recommended in an acute angle-closure crisis. It will be important to discuss with your ophthalmologist the best treatment option for you and your long-term follow-up plan.
Primary angle-closure suspects should have a discussion with their ophthalmologist about the risks and benefits of laser iridotomy, which is a procedure designed to prevent an acute angle-closure crisis. If you need to take medications that might increase your risk of having an attack or you have symptoms that suggest intermittent angle closure, this may push the balance towards undergoing this preventive procedure. Otherwise, sometimes it can be reasonable to follow-up over time to see if the angle becomes progressively more narrow.
Treatment for patients with primary angle-closure and primary angle-closure glaucoma involves removing a small portion of the outer edge of the iris using laser iridotomy. Patients who have an acute angle-closure crisis in one eye may have treatment performed in the other eye as a precautionary action, as they are at higher risk of having a similar event occurring in the other eye.
For more information of why an iridotomy helps prevent and/or treat an acute angle-closure crisis, please refer to a detailed article on this topic. Regardless of the specific diagnosis related to primary angle-closure you receive, it is important to discuss with your ophthalmologist the follow-up plan, because chronic forms of the disease can develop and it will be important to catch this earlier rather than later.
BrightFocus Foundation is a premier global nonprofit funder of research to defeat Alzheimer’s, macular degeneration, and glaucoma. Since its inception more than 50 years ago, BrightFocus and its flagship research programs—Alzheimer’s Disease Research, Macular Degeneration Research, and National Glaucoma Research—has awarded more than $330 million in research grants to scientists around the world, catalyzing thousands of scientific breakthroughs, life-enhancing treatments, and diagnostic tools. We also share the latest research findings, expert information, and resources to empower the millions impacted by these devastating diseases. Learn more at brightfocus.org.
Disclaimer: The information provided here is a public service of BrightFocus Foundation and is not intended to constitute medical advice. Please consult your physician for personalized medical, dietary, and/or exercise advice. Any medications or supplements should only be taken under medical supervision. BrightFocus Foundation does not endorse any medical products or therapies.
Encontrará recursos e información que ofrecen productos, servicios y otro tipo de apoyo para personas con glaucoma y sus familias.
In clinical trials, stem cell therapy for glaucoma shows promise for rebuilding the eye’s drainage system and protecting the optic nerve.
Resources and information that provide products, services, and other support for people with glaucoma and their families.
Join us for a fascinating conversation with Dr. Lucy Q. Shen as we explore cutting-edge research into restoring vision loss from glaucoma.
Support Groundbreaking Glaucoma Research
Your support helps fund critical research that could prevent vision loss, provide valuable information to the public, and cure this sight-stealing disease.
Donate Today

